The stories and adventures of a midwifery students in Seattle, WA traveling to Port Vila, Vanuatu for advanced training in midwifery and life. This blog collects contributions from students over the span of many years.
This is late in coming, but a little bit about Tanna (from Elias) --
Tanna is a small island in the south of Vanuatu, population 20,000, 212 square miles. There's a small hospital there, and as part of the Vancouver Island Vanuatu Partnership, a general practitioner from Vancouver Island staffs the hospital in 6-month stints. Dr David generously allowed me to tag along with him for a few days. While I haven't quiiiite written up that experience yet (which made a big impression), the other thing I did on the island was tag along with Geoff Mackley and Gareth Hawken, documentary film makers from New Zealand, who had set out to get the only HD footage of Mt Yusur (on Tanna) and the Ambrym Lava Lakes (on Ambrym).
Mt Yusur is one of the most accessible active volcanoes in the world -- you can climb right up to the rim! They had hired a guide so we were able to stop often along the way for them to get footage of the surrounding areas.
At the base of the volcano there are massive ash plains - totally foreign landscape.
There used to be a lake here, but in 2000, the lake burst through the valley, destroyed village of Sulphur Bay, and is now gone.
We met some folks who live in this village -- despite being entirely destroyed, nobody was killed -- and it's bizarre to think of geological things like this still happening. In my mind, geological phenomena are tens of thousands of years in the past. On the other hand, Vanuatu is an extremely tectonically active region -- I experienced two earthquakes in the 6 weeks I was there.
We hiked up well before any of the tour groups got there and got footage from the typical tourist vantage point. Then we hiked around to the far rim. The climb itself was not that bad -- one foot in front of the other -- but every so often I would realize where I was -- sheer mountain face on the left, sheer CANYON OF MOLTEN DOOM on the right -- and up my terror levels. It was worse when I realized we'd be hiking back in the dark. I ended up pulling on jeans over my shorts, not just because of jeans, but because I wanted some protection if I did end up falling down the side. The outside, at least. I was able to get some good photos of the explosions, but nothing like Geoff's cameras.
Just now Google emailed me to tell me my name popped up in this video! Geoff filmed a little interview piece of Gareth and me for NZ3 news. While Gareth was saying something about "this is the greatest show on earth, why would you want to sit at home watching television--" there was a HUGE eruption, which Geoff was able to swing around and capture. (He had asked me, "as a doctor, what's your advice to us on this volcano?" And he had dropped his radio and I had retrieved it from the skittering edge of the volcano, sooo...) Check it out!
Molly has since moved on to New Zealand, and I have since moved on to Australia. Check out my Vanuatu and Australia photos!
Monday, 9 Nov. Yesterday marked a momentous occasion in my stay here! Not only was it my 41st day (special only for its proximity to 42), but it was the first time I convinced anyone to try an upright position for pushing!
The women in our care here are equally afflicted by back labors and presumably posterior babies as our women back home. This is somewhat gratifying, because even though this is locally explained by laziness, it's probably not, and it means that there's not something we're doing especially wrong at home. (Or maybe we're all doing it wrong.) It's also super frustrating, because these back labors are long, difficult, feel very intense from the get-go, yet the contractions are poorly coordinated and somewhat ineffective. Iit's common to have someone coming in looking like very active labor and have her be at 2-3 cm. In fact, this weekend, we had a whole series who were at 2 cm for a full day! Logically we should send them home, because they're not in active labor. For various reasons this is not always possible, usually because they live far and don't have transport, and so we don't admit them but give them a bed in the extension ward. This leads to a feeling of still being in care though, with the accompanying requests for vaginal exams, which increases infection risk and frustration when the cervix is still 2 cm. I did send a few people home yesterday though! And one person "came back" only we hadn't discharged her and had no idea she was gone.
There are a number of positions that can facilitate a posterior or malpositioned baby to adjust his head position and make for an easier exit. These are usually assymetric and forward-leaning positions, and Penny Simkin's book The Labor Progress Handbook is invaluable for its illustrated suggestions. My success rate at recommending these positions is about 50%, I'd say. I usually demonstrate them for the family, my butt way up in the air, which has led to some photos (I want a copy of that, Amy!) and a lot of giggling. Some people can't be bothered, some are too tired already, some think they're just ridiculous, and some try them once or twice or only when I'm walking by.
My success rate at suggesting pushing positions, however, is like 2%. Most the midwives were trained in the flat-on-her-back school of pushing, grabbing one's legs or buttocks, holding the breath, and pushing pushing pushing. I never push it -- no pun intended -- but I suggest that she might want to try a squat, that it might be easier on hands and knees, that some people find they have more power kneeling, etc. It doesn't help that my limited Bislama -- and the apparent lack of word for 'squatting' in Bislama -- makes it difficult to explain what I'm talking about, leading to more instances of me climbing up on the adjoining bed and demonstrating.
S had back labor and a classic peanut-shaped belly, with lots of obvious fetal movement of small parts in front, suggesting the baby's back was along her back, facing front. This isn't always the case because babies are apparently like chubby owls and their bodies can be one way while their heads are basically the other, but still. She was pushing and making tiny progress, but it seemed like she'd greatly benefit from an upright position. When I suggested she try kneeling, and climbed up on the bed, hoisting up my gown to expose my knees, she actually did it! I couldn't believe it! And there was nobody around to yell at her and tell her to "slep strait!" just me and the student nurse who seemed delighted by this bizarre change in protocol. Once she'd gotten into position, I realized I had no idea how I would catch the baby. The delivery table was angled slightly, and I flitted from front to back trying to decide where would be the best place to be. There's a great birth video called Birth in the Squatting Position where babies just slide out onto the floor, and I've seen moms catch their own babies, so I knew it was entirely possible, but then I remembered a friend's thesis on obligate midwifery (based on the premise that babies are born facing back, requiring an attendant), and got confused. I figured it would sort itself out and positioned myself behind her as I had for the first couple babies I'd caught in the States, who were all born with their moms in hands and knees. Little by little, baby's head emerged, a millimeter at a time. It seemed painfully slow by Vanuatu standards, but this huge head -- part of a 3640g kiddo -- made it out with just the tiniest skid marks on the labia, no perineal tears at all! She was a primip, even! And the midwife who came in was delighted! She said maybe it was the first squatting birth in Vanuatu. I doubted this sincerely, but I hope the student nurse carries it forward -- she'll probably end up doing deliveries by herself in a small dispenary (clinic) on another island. (More about dispensaries when I finally get around to writing about my experience on Tanna.)
The rest of the day is a blur. The student nurse was on her way out when another mom was declared "fully" and she quickly had her baby. By the time I caught up with the paperwork on those two births, there were 3 more admissions, and two Australian med student friends came by to see if they could catch some births (since they're stationed on the med ward and haven't gotten the opportunity, I texted them to let them know we might have one that night). With them in tow, we managed a long, deep decel in a premature labor (thankfully resolved after adopting the open knee chest position, and hopefully the nifedipine stops her labor), a bunch more labor checks, some more admissions, and then two births! The first was a woman who'd been at 2 cm for 2 days and suddenly jumped to 8 cm with a very strong urge to push, and the next was a woman I'd sent home who came back at 9 cm and had a little boy! She also agreed to push in a kneeling position for a little while, and I think she ultimately delivered side-lying. I had a good time with Katie and David -- with Molly and Alex and Mel gone, and the Lycee students done with their observation, I've been missing having students to pal around with, especially those who will entertain my narrative teaching -- and they seemed happy to be deployed on various tasks and were quite helpful especially considering they insisted they'd only had a week of pregnancy so far. (I tried to go to Willy's presentation at his Lycee but missed it by a few hours, but he sent me his report! In French! Oh, the hilarity of my speaking French, especially throwing in Bislama words where my French fails.) I also feel like I've eased into new territory of feeling comfortable managing on my own, which is a nice feeling considering I've now finished my graduation requirements!
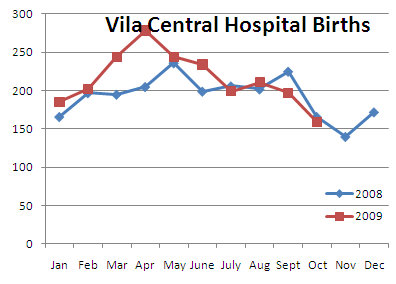
There was another woman who was ready to push right when I finished suturing the last one, but it was already midnight, the midwives were on their 3rd shift of the day, I'd been there for 14 hours, and we decided to go home. Pretty good day! And the busy-ness makes me think that maybe the October dry spell is broken. They only had 159 births in October. Pathetic! Why, back in April there were 278! And yes, I made a graph!
It's been a great couple of days- busy with nothing but goodness- and the first of our baby doc family has departed..... Liz and her hubby Craig headed back to Australia yesterday :( After sharing brunch at our favorite spot, La Tentation (don't be confused, we finally got to the bottom that this is not a misspelling nor the Bislama word for temptation, it is simply French), we said our goodbyes and the rest of us loaded up as the sailing crew on Cassiopeia. I steered as we sailed out towards our destination, where we dropped anchor, snorkeled and relaxed, and then as we tacked our way back into the harbor- no small job. I must say, weaving in between boats and buoys with a huge wooden sailboat can put a bit of pressure on a novice sailor. However, our captain commented that women are often much better at the helm, so I took that as a compliment for my ability to keep the wind in the sails and not hit any other boats, snorkelers, or reef! I was also pleased to see that no one appeared to be white knuckling their closest handrail.
As my time here in Vanuatu quickly comes to a close, time of course, feels like it is speeding up. Alex, Mel and I headed down through the quiet Sunday streets this morning to do one of our last dives together. These 2 baby docs and I completed our dive course together so we're trying to get a few more dives in before I take off next Sunday. We headed out to do a wreck dive.... my first, called Konanda. This was a 45 meter ship badly damaged by Cyclone Uma in 1987. It is still intact (including some mugs and a tea pot on the top deck) and overall was just a fun dive to be able to explore the nooks and crannies of an old boat underwater. After finishing that dive, we headed to another site to join in on some environmental restoration at a popular dive and snorkeling site. There is an invasive species that is populating the reefs here, called the crown of thorns, and we spent a couple of hours rounding them up into bags, in which they will spend their last moments in the sea. I worked with one of the Ni-Vanuatu dive instructors, Jerry, and we floated above beautiful coral and fish, scanning for the infamous circular and spiky creatures. Jerry had the tool for spearing them, while I carried the bags and together we championed the cleanup effort, collecting 73 crown of thorns! After an afternoon of diving, a gray sky, and a cool breeze, my lips were blue and I was chilled to the core, even though the water is a pleasant 24 or 25 degrees Celsius, 3 hours even with a shortie wet suit makes for some shivering. After a hot shower, finally starting to warm up! The company that I have been diving with is called Big Blue and for those coming to Vanuatu I would highly, highly recommend them. http://www.bigbluevanuatu.com/. Tell them you're volunteering in the hospital and you get the local discount! Very nice! Good fun and fabulous people.
On our long boat ride back into Vila, I was reflecting about what I've appreciated most about the people here.... and undoubtedly what I will miss! First of all, many of the Ni-Vans wear flowers behind their ears- men and women- in the market, playing volleyball, coming in to give birth..... it's beautiful. Secondly, the people of Vanuatu exude happiness and are amazingly friendly. Walking down the street children and adults, men and women, say hello, good morning, good night..... some sort of acknowledgment, and sometimes going out of their way to do so. The people I have worked the closest with here are the midwives and the dive crew and all of these folks fill the interactions with laughing, cracking jokes, smiling, and generally enjoying what they are doing. Beautiful people, truly, inside and out, who will flash you a smile and give you a pat on the back or grab hold of your hand when they see you. It's particularly notable because although life here appears more simple and functions on Island time, it is in no way to say that it is easy. I think many of our prior posts can attest to this.
As for births this week, I caught a couple more babes.... another Star-gazer baby! Silly little one, she came out facing up and had her cord all wrapped around her neck and her shoulder and belly....but pink and crying in no time. After wiping off the babe and moving her to the warmer, I turned around to see that the mom was bleeding.... quite a gush, about 200ml.... separation gush.....and soon out came her placenta- Duncan style. This is when the part of the placenta that is attached to the uterus (rather than the side the baby is snuggled up against)is what you see when the placenta arrives. Most often the placenta flips in on itself so that the shiny part where the umbilical cord inserts is what you see when it comes out, and you have to flip it inside out to see the other, maternal, side. In the 130 or so births I have attended in my lifetime, I can recall 3 placentas coming out Duncan. I always thought it mostly had to do with being a low-lying placenta, but Elias did some reading and sounds like it can be a sign of other things to come, mostly a hemorrhage, which this mom did have. Her total blood loss was about 600ml, not frightening by our U.S. standards, but since the women here bleed so little since they all receive the antihemorrhage meds after birth, 600mls is concerning, especially since this mom also received those meds and she still bled. An IV with even more syntocin got it all under control and made for a very firm uterus. She had a small first degree tear that was easily sutured and was the first suture job here that I really felt great about- my skills are improving!
This week I also observed my first VBAC (vaginal birth after cesarean) birth..... my first here and anywhere, since so few out of hospital midwives in Seattle do them anymore since malpractice insurance in Washington doesn't cover VBACs. This mom told me that she really wanted to experience the pains of giving birth to know what it felt like after having to have a Cesar with her firstborn in 2004. I can understand that, as I would feel the same way since giving birth vaginally is so central to our female anatomy and physiology and for some, seemingly tied to female identity .... the ability to create and sustain a baby, to give birth, and to feed the babe....it's amazing the design, and one of those things I just absolutely want to experience. And so did she.... and she did it! After 2 hours of pushing, an episiotomy and lots of help getting the babe's head born, her sweet daughter was born vaginally. Strong mama, strong baby! 3.3kg, healthy and hungry as could be! And both mom and babe settled in for a long afternoon nap.
And on that note, speaking of nap.... off to get some much-needed sleep. Elias is already in bed, his eyes begging me to turn off the light so darkness and good sleep can reign. Hope to post some photos on this one tomorrow.
I'm sitting at our little table in our cozy studio, just finished a bowl of chicken and vegetable soup. Sounds strange to be eating that here in the South Pacific, eh? Well, today is the perfect recovery day as it is gray and rainy outside and I was at the hospital into the wee hours of the morning, so needless to say, it's a slow morning. Filled perfectly by homemade chicken soup.
A busy night at the hospital last night. It started with the phone ringing in the maternity ward, which I have gradually acquired the confidence to answer as my Bislama has improved. “There is a lady coming” was all that the voice said. In walked a young woman teetering on active labor with her first babe. I checked her and her cervix was very favorable for labor: 3cm, very thin, with a well-applied head that was nicely engaged in her pelvis. After checking the babe’s heart rate and monitoring her contractions, all the while rubbing her back and offering reassurance as best we could, we made her a bed and encouraged her to walkabout, drink plenty, and eat if she liked and to tell us when she felt like pushing.
Then before we were even finished cleaning up the Admission room, in walked another woman in early labor. This woman falls into the category of grand multip (as many women here in Vanuatu do since it’s so common to have lots of babies), pregnant with her 5th babe. She reported some bloody show the night before and that morning and said she recently started feeling some mild pains. I checked her and found that her cervix was very soft and stretchy, but only 2cm dilated, at least 1cm thick, and the babe was well engaged. Now if the first time mom who had come in had had a cervix like that we probably would have sent her home to continue laboring and thin and dilate the cervix since that’s a lot of the work of early labor (unless she lives far away), but with a multip, a grand multip at that, that would be a big mistake for things can move very quickly, even with a cervix that is thick and not very dilated. And so as this mom laid on the exam table while we did a tracing of the babe’s heartbeat, she had 5 good strong contractions . I thought, yes, grand multips, they keep you on your toes. Never assume anything and trust the mom's instincts. This mom knew today was the day.
After we encouraged the experienced mom to walkabout and provided her with a bed in the antenatal room, I went to the tea room to have some dinner and watch some French soap operas I'm not a big TV person in general (on second thought, perhaps that is an understatement, being that I haven't had a television for over 10 years now), and I can't understand French, but it's interesting to try to pick up what I can from the body language and intonation. Never a shortage of those soaps on the little TV that plays continuously, 24 hours per day. As I walked back to the front desk, a woman greeted me and pointed down the hall saying she’s ready. I thought she was pointing to the first time mom, but then noticed a new belly in the hall, and blood dripping all over the floor. Oh no, I thought, this does not look good. Too much blood before the baby has arrived.
We took her right into the birthing theatre, she climbed up onto the table and her dress was soaked in blood, blood stained the insides of both her legs. It all happened so fast that we got her name, that this was her second baby, but didn’t have time to pull her chart. I asked one of the baby docs with me to check in on the babe’s heartrate while I gloved up to do an exam. To my surprise and relief, the babe’s heart rate was pleasantly beating away in the 140’s. I checked the mom’s pulse to be sure we weren’t just picking up her heartbeat- 120. Okay, I thought, where is all this blood coming from? Placental abruption (separation)? Placenta Previa (low-lying)? Hmmmm...... Large clots of blood passed my fingers as I started the exam. Inside there was no cervix, she was completely dilated and she had a bulging bag of water. I couldn't feel any placenta either, luckily. I debated, to rupture her membranes or not….. I considered this situation with all the bleeding and decided I wanted to know what color the fluid was. So we ruptured her waters (or “released” the membranes as some prefer) and not surprisingly, it was bloody. Well, little more information that provided, but the babe’s heartrate continued beating away without any decelerations. It’s interesting to observe how when some women are complete there is no stopping their urge to push, while others seem to have no urge, and still others have the dreaded premature urge to push before the cervix is fully dilated. This mom fell into the second category, so we coached her on pushing when her belly was sore. She pushed and pushed with all her might, and slowly, slowly the head made it’s way down. And I do mean slowly, as she would take a deep breath, hold it while pushing for 15 or 20 seconds and the head would move millimeters. And it appeared to me that she had had some sort of repair after her first birth because the tissue just inside the vaginal opening was very tight- unnaturally unable to stretch. Finally the baby started crowning and I saw his little face, pale and void, followed by a pale, limp body. To see a babe’s face as he is crowning in a woman laying flat on her back means that her baby was born face-up, or posterior, or face-to-pubes as they call it here. I like to fondly refer to these babies as star-gazers. This position however, generally makes for a more difficult labor, or at least a longer pushing stage in my experience, hence the slow, slow descent.
I stimulated him and was conscious of not cutting his cord right away, knowing that he was still getting some oxygen from the placenta, so long as the cord was still pulsing. (In the States as midwives we generally always do delayed cord clamping, waiting until the pulsation stops, but not so here.) After close to a minute, with no grimace, no effort to breathe, no tone, and no color, I clamped and cut the cord so we could take his little body over to the warmer and work on getting him to breathe. The midwife suctioned him and I grabbed the bag to help inflate his little lungs. I could feel a good heart rate through his chest, confirmed by the little rhythmic beatings I heard with the stethoscope. Still no breath. A few inflation breaths made his little chest rise and shortly thereafter he started breathing, shallowly. His eyes were still closed, and overall he appeared to be teetering in and out of his body. Come into your body little one, tell us about how hard that was with a nice good cry, I thought. We put him under the plastic head box with oxygen and slowly, slowly, over the course of 20 minutes or so, he came into his body. His eyes shifted slowly this way and that. His heart rate remained good and his color improved. The last to improve was his tone. His APGAR scores were 2 at 1 minute, 7 at 5 minutes, and 8 at 10 minutes. Not great, but alive, and improving with time. He weighed 2.6kg. When put to the breast he sucked weakly a few times, then he’d go back to sleep. He seemed oh so sleepy. Clearly a difficult transition for him. This was one baby that I wanted to hear wail and scream, who never let us hear his little voice. It wasn’t until later that I scanned the mother's chart and found that her due date was not until 27 November (although due dates are to be taken with a grain of salt here as they can be imprecise), so it’s possible that this guy was just early and therefore his lungs and sucking muscles were not quite developed.
We never did find out where all the blood came from. The placenta was completely normal and came out Schultz (whereas a low-lying placenta ha a greater chance of coming out Duncan- fancy words describing which side of the placenta is showing when it comes out). Maybe her cervix dilated so quickly that all the cervical capillaries just burst? Not sure, but that was a lot of blood, whatever it was...
Due to the nature of the tight tissues, this mom ended up with a ragged second degree tear that included a pocket just inside her vagina and a lateral vaginal/perineal split, which I actually thought was a third degree because I saw a little piece of the famous shiny anal sphincter. The midwife stepped in and sewed her up, which was fine because meanwhile our first time mom was grunting next door.
She gave birth with ease and I sutured her bottom while her big healthy girl with a strong pair of lungs reminded us of how quiet the little guy next door was.
Meanwhile, we had another first time mom come in in early labor so we admitted her and sat down to get caught up on all the paperwork.
As the night continued the grand multip made some more noise and her eldest daughter who was continually rubbing her back and giving her water said it was time. I checked her and was surprised to feel just how much cervix was left….. she was 7 cm and the front part of the cervix was thicker than the sides or the back. This mom was really feeling it in her back, so I thought, hmmm, maybe this is a night of posterior babies. Based on my experience here with grand multips, I have had a few moms that wanted to push and they were 8cms or so, and with just one or two good pushes, the cervix was gone and the baby's head was on the perineum. I asked her to give a good push just to see what happened, but the cervix did not give. At this point it was about 9:45pm. She had progressed 5 cms in just over 3 hours- great progress. So I encouraged her to breathe through the contractions and to walkabout. An hour later, she wanted to push again, so I checked her and she was essentially the same, although the front part of her cervix was slightly larger than during the last exam. I encouraged her to lay on her side for a few contractions, then switch to her other side, hoping that would help with her cervix. Another hour, another strong urge to push.... another exam, essentially the same dilation, with an even thicker anterior cervix. Where is my homeopathic Arnica, I wondered.... in my first aid kit 2 blocks away. DARN! Once again, I encouraged her to push and she if I could hold the cervix back over the babe's head. No luck. We ruptured her membranes to see if the head could be better applied and waited another hour. Still the same, however, the front of the cervix had swollen to something like a thin sausage. I had never felt such an anterior lip and it was really something. This is why the premature urge to push can be disastrous because the cervix can swell to the point that it can't be pushed back and if it gets really bad the blood supply can get cut off and the cervix can be shed. Well I hoped we weren't heading down that road, so I called the midwife in and she also tried to reduce the lip. No luck, it was too big. We turned the mom on her side and once again encouraged her to breathe through the contractions to try to prevent further swelling. We decided to call the OB on call. It was 1am and this wasn't an OB we were particularly thrilled about, but we were out of ideas between the 3 of us. Meanwhile the mom was unable to control her urge to push and was wildly pushing with each contraction, still laying on her side. Just after hanging up the phone with the OB, we checked her again and low and behold, that big fat cervix was nowhere to be found. Amazing. Sidelying pushing had done it. We quickly rang the OB and told her not to come and within 5 minutes she pushed her baby out, not posterior (at least not at this point). A 3.4kg baby girl, with healthy lungs and a loud cry swam out of her mama all at once. This placenta was the largest that I had seen here. Pretty flat, but just huge- like the largest of large pizzas you've seen. It must have covered a good portion of her uterus inside! No suturing needed, but I did see a big purple bulge further up in her vagina- the swollen cervix, congested with blood. Luckily she had minimal bleeding so even her cervix appeared intact.
A lesson learned, grand multips keep you on your toes for lots of reasons- always a higher risk for hemorrhage, labors can be quick and unpredictable, or apparently longer and plateauing. And surprisingly to me, even the grand multips cervix can swell, into an anterior lip beyond any anterior lip I had ever felt before. And in the end, a combination of position and the mother following her uncontrollable instinct to push was what got her babe past that hurdle and into her arms. Whew!
I cleaned up and ran home to a quick shower and tumbled into bed exhausted, reminded of the many late nights I had kept during my training in Seattle. But also honored by the beauty of seeing a woman through the entirety of her birthing process, the challenges and the joys, and welcoming a few more little Ni-Vans into the world.
Welcome! Follow along with Kat and Elias over the coming week in Port Vila, Vanuatu as we share our experiences of a new place and culture, working in the local hospital, and catching babies!